

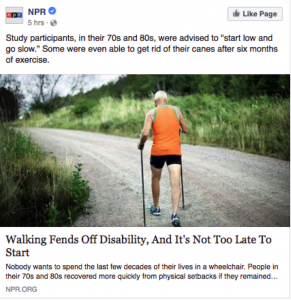
NPR caught flak from the disability community this week as they published an article reporting on a medical study supporting physical activity as a means of delaying or preventing mobility impairment in sedentary seniors. “Nobody wants to spend the last few decades of their lives in a wheelchair,” NPR’s caption, since edited, declared. “LOL guess I missed the boat here. Oh well. ¯\_(ツ)_/¯” activist Emily Ladau snarked. “Anyone can become disabled at any given time,” another wheelchair user pointed out. “Just say exercise is healthy. Don’t drag us disabled people into it.”
There are so many ways in which health coverage can be more sensitive and aware of a disabled audience—and we are part of the audience of health coverage, despite the implicit assumption of many articles that journalists are writing for a nondisabled audience. Language, while important and indicative of a writer’s attitude toward the subject, is only one element of disability-aware health coverage, and I recommend, as I do to everyone who publishes about disability, the National Center for Disability and Journalism’s style guide, which covers many aspects of disability typically not mentioned in AP or in-house style guides.
The sad reality is that much of our medical system, which by rights should be one of the most supportive environments to disabled people, is instead one of the most hostile and stigmatizing. This extends to medical research as well, where implicit bias against disability and disabled people impact everything from study design to topics chosen for study in the first place, as this study illustrates all too well—more on that below.
This is why it’s particularly important to the disability community that coverage about medical studies be critical and aware of that pre-existing bias in scientific research. Health journalists exercise discretion in choosing which studies to cover, the people whom they contact to get quotes for commentary, and the angle with which they explain the significance of the study and identify any limitations (or use quotes from others who do so).
So when I look at a piece like this, I see a few different things: reporting that only quotes scientists and healthcare providers, not disabled people or seniors themselves, and the choice to uncritically cover a study that had significant anti-disability bias baked in.
Most health coverage I read includes quotes primarily from healthcare providers and researchers. In disability advocacy, we like to say “nothing about us without us,” so it is frustrating that we so rarely see members of our community contributing to stories that are ultimately about our disabled bodies. In doing so, physicians and researchers, rather than disabled people ourselves, are established as the only sources of authority on our bodies, with troubling ramifications.
So now let’s break down some of the problems I have with this study—problems that readers relying on this article to understand the finding would not necessarily have seen.
A bad yardstick for measuring outcomes
The first red flag, if not outright problem, in the study is using mobility as such as a health outcome. The study’s abstract, as well as the introduction, point out that mobility impairment is a risk factor for hospitalization, morbidity, and mortality. The study’s authors identify ambulatory mobility as a critical element of function and independence, yet there is no recognition of why that is, nor would one expect it from the kind of medical-model thinking pervasive throughout medical research. When a study’s authors conflate ambulatory mobility with high quality of life, as they do here, it is clear to me that they have implicit bias against disability.
Some studies are paradigm-shifting, while others are about creating a body of evidence to confirm a widely-held hypothesis. This study is clearly the latter: it is a straightforward “exercise maintains physical function more than merely talking about health” finding, specific in this case to an older population. Anyone familiar with the athletic “principle of specificity” knows that if you want to train a specific skill, you do that skill often. It is completely intuitive to me that walking and doing accessory training to facilitate walking maintained this population’s ability to walk. As the study admits, it did not quite have the statistical power to demonstrate a reduction in “major mobility disability,” so that outcome was not statistically significant; even so, I certainly buy that this sort of intervention would do so.
But there is a significant element of the study missing from NPR’s coverage: hospitalizations did not decrease in the physical activity group, nor did mortality. This means that the maintained mobility did not decrease the major health outcome for which reduced mobility is a risk factor. Reduced risk of morbidity, mortality, and hospitalization is, by the study’s own admission, the importance of maintaining ambulatory mobility. As far as this specific study is concerned (and I acknowledge it is only one part of a larger body of literature), the physical activity intervention they performed only improved ambulatory mobility, not health. The ability to walk is not synonymous with health. It is not synonymous with quality of life. The assumption that they are is, quite frankly, ableism in its purest form.
I am a disabled athlete. I train 8-10 hours a week, have competed internationally in swimming, and am beginning training for competition in wheelchair racing in order to attend Paralympic Track and Field nationals next year in the 100m dash. So clearly, one doesn’t need to sell me on the benefits of physical activity. But the important thing to note there is that I do all of those things and am highly physically active while still having a major mobility disability. I certainly cannot walk 400m; on my best day, I could perhaps walk 4 or 5 steps. Prior to wheelchair use, I was as sedentary as this study might define it because I could not ambulate adequately to perform regular physical activity. I am active because, not despite, of my wheelchair use, and I am not alone.
Does disability really equal inactivity?
This brings me to a serious problem pervasive throughout medical research, that use of assistive devices suggests a decrease in physical activity and is therefore a categorically undesirable outcome to be avoided. This story propagates this stigma, not only in the now-revised caption on the story, but in the Facebook caption for this story and story itself, which frame elimination of cane use as a cause for jubilation (possibly the case in the studied population, but we only have the study author’s word on it, since again, no seniors or disabled people were quoted in the piece). This stigma discourages people from seeking appropriate mobility equipment, and to ditch said equipment if it’s even remotely possible. Little thought is given to the potential benefits of continued mobility device use. Even less attention and funding is devoted to research on physical activity in disabled young and older adults, let alone a rigorous examination of the tradeoffs in physical activity and mobility device use and how that affects health outcomes.
I am not arguing that ambulatory mobility is not worthwhile or that these study participants should plop themselves in a wheelchair at the first sign of reduced mobility, only that physical activity can be presented as a worthwhile endeavor regardless of mobility level, that mobility disabilities (and by extension, the people who have them) should not be stigmatized or used as a fear tactic to encourage exercise, and that we should support policies and interventions that allow seniors and all disabled people to be physically active. Mobility is not an intrinsic good: it is an instrumental good to enable independence and autonomy and reduce the risk of bad health outcomes and death. There are many ways to achieve those ends, and we should not allow ableist bias to arbitrarily constrict our options and discourage people from utilizing mobility tools to be active and present members of our communities.
What price mobility?
The quality of mobility devices available to older populations is certainly a part of the “lack of independence and function” this study and others attribute to a major mobility disability. Here is a side-by-side of the kind of wheelchair ubiquitous among seniors next to a picture of me in my own.


The one on the left looks all too familiar to most people, but seniors almost never receive high-quality, ultralightweight chairs like the one on the right when they are prescribed a manual wheelchair. A standard or “hospital” chair weighs 64% more than mine and is not fitted to the individual. I would struggle to propel one of those clunky tanks and would likely be unable to continue my own level of independence and function, and I’m an athlete. How much more so would a senior, often with significantly less muscle mass than I have and a lower capacity for intense physical activity, lose independence when provided with a wheelchair that’s utterly unfit for long-term use? That is not a function of the mobility impairment, but of healthcare policy that prescribes inadequate equipment. It is the very illustration of the social model of disability, where barriers do not solely stem not from the medical impairment, but from policies, environments, and attitudes that prevent disabled people’s full participation in society.
And so, with recognition of the role of social and healthcare policy in mobility and physical activity, we come to my final complaint with health journalism as embodied by this article: inadequate emphasis on policy as a contributor to health outcomes. I do not speak here of public health, which has its own problems but does leverage policy as a vehicle of improving health, but rather of reporting on clinical studies about health interventions on an individual scale. It is not the medical researcher’s job necessarily to discuss social factors in health—medical studies examine targeted hypotheses—but it is the job of a writer whose job it is to explain the significance of those studies to our daily lives. When journalists act as uncritical stenographers for medical researchers, not only do they propagate the biases endemic to that community, but they deprive the public of the kind of analysis and discussion that physicians and scientists perform when presenting papers among their colleagues in medical schools and labs across the country.
Health reporters are the primary contributors to medical fluency and public understanding of health in our society, and they must do their jobs with respect for that enormous responsibility. That means choosing the studies they cover with care, and performing that coverage with an approach that is both critical of the material and inclusive of all stakeholders, not just healthcare professionals, but the people whom medical interventions most impact: us.
Photo: Sam de Leve/All Rights Reserved
Thank you for Sharing.
I also feel there is an implicit ageism in assigning old people, old equipment as if that is their due.